This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whatsoever.
Patient came with cheif complaints of burning type of sensation of whole body since 1 week.
Fever since 1 day
HOPI:
Patient was apparently asymptomatic 2 months back after which he had an RTA during which he had cervical cord stenosis and was operated with cervical cord laminectomy i/v/o weakness of both upper and lower limbs. After which patient was on physiotherapy and power improved gradually.Now patient had h/o burning sensation and numbness of whole body( paresthesia).
He also have complaints of fever since today afternoon associated with chills , relieved on medication.
H/o of burning micturition since 4-5 days
No H/o decreased sensations
No h/o bowel and bladder incontinence.
No h/o seizure activity
No H/O cold, cough, sore throat
No H/o nausea , vomiting, pain abdomen
No H/o loose stools
PAST HISTORY:
Not a k/c/o dmII, htn, thyroid disorders,asthma,epilepsy
GENERAL EXAMINATION:
Patient is conscious, coherent
No pallor, icterus, cyanosis, clubbing, lymphadenopathy, edema,
Temp: 101.5 degree F
Pr: 98bpm
Rr: 20cpm
Bp:130/70mm Hg
Grbs:151mg/dl
SYSTEMIC EXAMINATION
Cvs:S1 S2 heard , No murmurs
Rs: BAE +, NVBS
P/A: NT
CNS:
Tone UL LL
R N N
L N N
Power : UL LL
R 2/5 4/5
L 3/5 4/5
Reflexes - B T S K A P
RT- +3 +3 2+ 3+ 3+ F
LT- +3 +3 2+ 3+ 3+ F
INVESTIGATIONS:
4/6/23
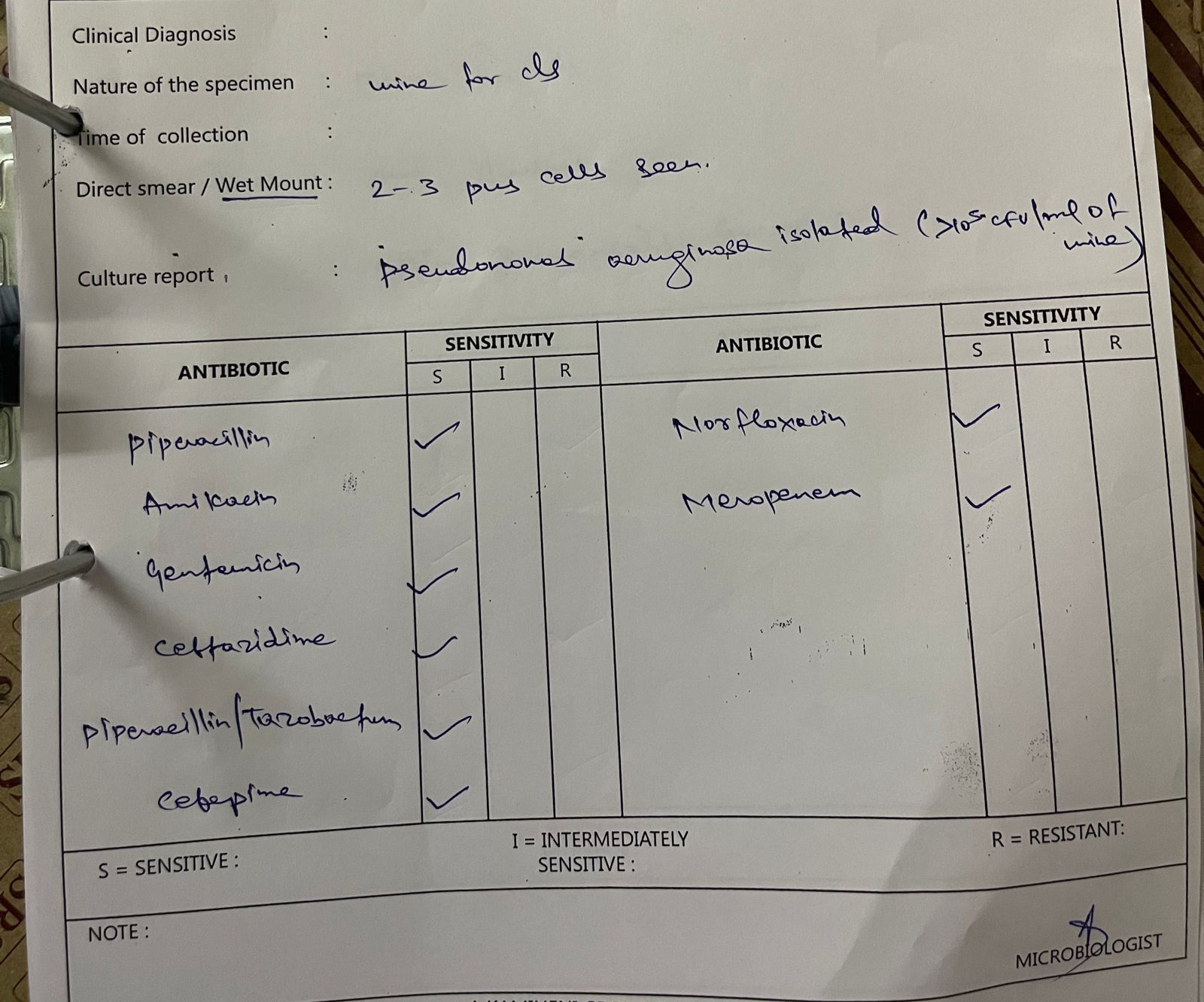
Culture:
DIAGNOSIS:
Pyrexia under evaluation with cervical laminectomy 2 months back
TREATMENT:
1. Inj Neomol 1 GM iv/sos ( if temp > 101 F)
2. Inj Monocef 1 GM iv/ bd
3. Inj optineuron 1 amp in 500ml NS /OD
4. Tab dolo 650mg Po/ Sos
5.tab pregabalin 75mg po/Hs
























Comments
Post a Comment