GENERAL MEDICINE
GENERAL MEDICINE.
M.YASHWITHA.
ROLL.NO:73.
35 F WITH AKI ON CKD
A 35 year female, resident of manipaka, came to casualty with complaints of bilateral pedal edema since 20 days,decreased urine output since 20 days,Facial puffiness , shortness of breath ( a/w orthopnea and PND ) ..
H/O fever spike +, 10 days back, not associated with chills and rigor, subsided on taking medication.
C/o cough with expectoration, (yellowish in colour).
Pt was apparently asymptomatic 2 months back then she developed chest pain for which she visited local hospital in miryalaguda , on evaluation she was diagnosed to have chronic kidney disease and low hemoglobin, 2PRBC Transfusions were done
After PRBC transfusion she developed b/l pedal edema, which subsided on medication.,
• 20 days back she developed b/l pedal edema, reduced urine output, sob a/w orthopnea, and PND, and facial puffiness.
•10 days back she developed fever a/w chills and rigor, which subsided on medication.1 PRBC transfusion done in Nalgonda hospital yesterday.
K/c/o HTN since 3 year's
Not a k/c/o DM, asthma, TB.
On Examination:
pt is c/c/c,
Pallor -present
Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadenopathy - absent
Pedal edema - b/l present



Vitals:
Afebrile
Bp: 170/100 mm hg
PR: 99 bpm
RR: 22 cpm
SpO2: 87% @RA
CVS: S1,S2 +
RS: BAE+
P/A: SOFT, NON TENDER
CNS: NAD
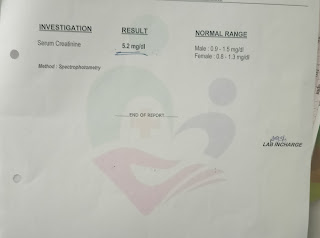
Outside reports on 30/11/21:









2/12/21:

PROVISIONAL DIAGNOSIS:
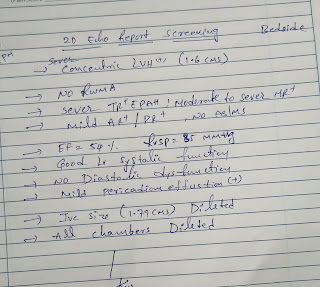
AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months.
Plan of care:
1. Head end elevation upto 30'
2. O2 supplementation if SpO2 < 90%
3. Inj. Lasix 40mg iv tid
4. Inj. PIPTAZ 2.25gms IV BD ( D1)
5. TAB. NICARDIA 10MG PO BD
6. TAB. NODOSIS 550MG PO BD
7. TAB. SHELCAL 500 MG PO OD
8. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
9. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
10. SYP. ASCORYL PO TID
11. HRLY VITALS MONITORING.
Day 2:
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
Pt shifted to CKD ward
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
VITALS:
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2. O2 supplementation if SpO2 < 90%
3. Inj. Lasix 40mg iv tid
4. Inj. PIPTAZ 2.25gms IV BD ( D2)
5. TAB. NICARDIA 10MG PO BD
6. TAB. NODOSIS 550MG PO BD
7. Tab. Orofer XT PO/OD
8. TAB. SHELCAL 500 MG PO OD
9. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
10. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
11. Inj. Iron sucrose 1 amp in 100ml NS
12. SYP. ASCORYL PO TID
13. HRLY VITALS MONITORING
On 18 /12/21:

On 19/12/21

On 20/12/21

Day 3:
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
Pt shifted to CKD ward
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
VITALS:
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2 .Inj. Lasix 40mg iv tid
3. TAB. NICARDIA 10MG PO BD
4. TAB. NODOSIS 550MG PO BD
5. Tab. Orofer XT PO/OD
6. TAB. SHELCAL 500 MG PO OD
7. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
8. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
9. Inj. Iron sucrose 1 amp in 100ml NS
Day:4
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
In CKD WARD
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2 .Inj. Lasix 40mg iv tid
3. TAB. NICARDIA 10MG PO BD
4. TAB. NODOSIS 550MG PO BD
5. Tab. Orofer XT PO/OD
6. TAB. SHELCAL 500 MG PO OD
7. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
8. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
9. Inj. Iron sucrose 1 amp in 100ml NS
35 F WITH AKI ON CKD
A 35 year female, resident of manipaka, came to casualty with
c/o b/l pedal edema since 20 days,
decreased urine output since 20 days,
Facial puffiness , shortness of breath ( a/w orthopnea and PND )
H/O fever spike +, 10 days back, not associated with chills and rigor, subsided on taking medication.
C/o cough with expectoration, yellowish in colour,
Pt was apparently asymptomatic 2 months back then she developed chest pain for which she visited local hospital in miryalaguda , on evaluation she was diagnosed to have chronic kidney disease and low hemoglobin, 2PRBC Transfusions were done
After PRBC transfusion she developed b/l pedal edema, which subsided on medication.,
20 days back she developed b/l pedal edema, reduced urine output, sob a/w orthopnea, and PND, and facial puffiness.
10 days back she developed fever a/w chills and rigor, which subsided on medication.
1 PRBC transfusion done in Nalgonda hospital yesterday.
K/c/o HTN since 3 year's
Not a k/c/o DM, asthma, TB.
O/E :
pt is c/c/c,
Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadenopathy - absent
Pedal edema - b/l present
Vitals:
Afebrile
Bp: 170/100 mm hg
PR: 99 bpm
RR: 22 cpm
SpO2: 87% @RA
CVS: S1,S2 +
RS: BAE+
P/A: SOFT, NON TENDER
CNS: NAD
Outside reports on 30/11/21:
PD: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months.
Plan of care:
1. Head end elevation upto 30'
2. O2 supplementation if SpO2 < 90%
3. Inj. Lasix 40mg iv tid
4. Inj. PIPTAZ 2.25gms IV BD ( D1)
5. TAB. NICARDIA 10MG PO BD
6. TAB. NODOSIS 550MG PO BD
7. TAB. SHELCAL 500 MG PO OD
8. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
9. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
10. SYP. ASCORYL PO TID
11. HRLY VITALS MONITORING.
Day 2:
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
Pt shifted to CKD ward
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2. O2 supplementation if SpO2 < 90%
3. Inj. Lasix 40mg iv tid
4. Inj. PIPTAZ 2.25gms IV BD ( D2)
5. TAB. NICARDIA 10MG PO BD
6. TAB. NODOSIS 550MG PO BD
7. Tab. Orofer XT PO/OD
8. TAB. SHELCAL 500 MG PO OD
9. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
10. INJ. ERYTHROPOIETIN 4000
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
Pt shifted to CKD ward
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2 .Inj. Lasix 40mg iv tid
3. TAB. NICARDIA 10MG PO BD
4. TAB. NODOSIS 550MG PO BD
5. Tab. Orofer XT PO/OD
6. TAB. SHELCAL 500 MG PO OD
7. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
8. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
9. Inj. Iron sucrose 1 amp in 100ml NS
Day:4
https://elogformedicalcasebyintern.blogspot.com/2021/12/35-f-with-aki-on-ckd.html
In CKD WARD
35 year old female
S:
Sob reduced
Pedal edema reduced
O:
Pt is c/c/c
Pallor +
B/l Pedal edema +
No icterus, cyanosis, clubbing, lymphadenopathy
Afebrile
Bp: 160/80 mm hg
PR: 88 bpm
RR: 22 cpm
SpO2: 92% @RA
CVS: S1,S2 +
RS: BAE+, decreased breathsounds in b/l ISA, MSA
P/A: SOFT, NON TENDER
CNS: NAD
A: AKI ON CKD (stage v), with egfr: 5ml/hr, with metabolic acidosis ( resolving ), with b/l pleural effusion with k/c/o HTN since 10 months
P:
1. Head end elevation upto 30'
2 .Inj. Lasix 40mg iv tid
3. TAB. NICARDIA 10MG PO BD
4. TAB. NODOSIS 550MG PO BD
5. Tab. Orofer XT PO/OD
6. TAB. SHELCAL 500 MG PO OD
7. NEB. WITH SALBUTAMOL 2 RESIPULES / 4TH HRLY,
8. INJ. ERYTHROPOIETIN 4000 IU S/C WEEKLY ONCE
9. Inj. Iron sucrose 1 amp in 100ml NS



{kind=link}
Comments
Post a Comment